Quantifying health outcomes is now a standard phenomenon, and the maternal mortality ratio (MMR) has become one of the major measurements with a wide range of uses. It is utilized to assess not only the state of maternal health but also health systems functioning, gender in/equality, and beyond. As of late, it is also serving as a human rights indicator for such rights as life and health. Despite its growing importance, however, the processes that produce such data do not attract the attention they merit. This blog highlights some aspects of the challenge.
Mulu Beyene Kidanemariam - Mulu.kidanemariam@uib.no
PhD Candidate at the Faculty of Law, University of Bergen, Norway
Mulu studied law in Ethiopia and is currently working on a PhD project that examines the legal dimension of a maternal death auditing system. He stayed with CORTH in autumn 2022 as a visiting student.
Following the prominence of ‘evidence-based decisions making’ in the 1990s, quantification of developmental outcomes, including health, has become commonplace. Maternal mortality ratio (MMR), which principally represents the population-level risk of women dying in relation to childbirth, is among the health indicators that have come to acquire great visibility at both domestic and global stages.
Currently, the MMR is an indicator for the maternal health goal under the SDGs. It is also widely regarded as a marker of the overall health system functioning and the state of gender equality. As such, MMR numbers are among the considerations used in developing health policies in both national and global settings. Such metrics, moreover, form part of the criteria utilized by certain international loan schemes as well as in national budget allocation. Human rights monitoring organs also use MMRs, initially to assess the progressive realization of health rights and recently as a proxy indicator, not only of sexual and reproductive health rights, but also of the right to life, freedom from violence against women, and freedom from discrimination. The growing importance and multiple uses of the MMR is thus evident.
The WHO defines MMR as the number of maternal deaths per 100,000 live births. Maternal death, in turn, refers to the death of women related to or aggravated by the pregnancy or its management. These definitions give the impression that country-specific MMR numbers that is often seen in reports and studies alike result from a technical head count of deaths and live births during a given time.
This is not the case in practice, primarily because about a third of all countries globally lack robust vital statistics registration systems, the most reliable data source, to capture these figures. And many of those that lack such systems are countries with an apparently high burden of maternal deaths. As a result, statistical models and approximation methods are employed to estimate maternal mortality levels for a great number of countries.
In constructing the estimations, international institutions often use covariates such as GDPs, fertility rates, and the number of skilled birth attendants. The WHO and other agencies use these values to both produce new estimations where no data on maternal death exists and to ‘smoothen’ incomplete data that countries report.
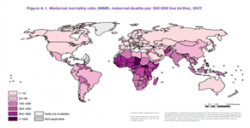 WHO et al (2019) Trends in Maternal Mortality: 2000-2017
WHO et al (2019) Trends in Maternal Mortality: 2000-2017
Such estimations are fraught with limitations. Among others, the relevance and sufficiency of the covariance used to represent the risk of maternal death is questioned. For instance, the list leaves out critical determinants of maternal health risks such as political stability, gender inequality, health budget, and quality of care. Many of the covariates are, indeed, estimations themselves. Thus, the numbers can merely tell partial stories, as Wendland (2022) has phrased it. Without representing realities, the estimations are less likely to help the countries concerned develop effective health interventions. Furthermore, it has been argued that these estimations primarily cater to the needs of international organs and donors, and in the process remove attention from the crucial need to foster nationally owned health information systems.
These shortcomings are fairly acknowledged. The understanding thus is that the estimations are interim measures to be used only until countries develop national health information systems capable of reliably measuring actual maternal mortality numbers, and efforts are being exerted to develop national routine information systems. In the meantime, the production of estimations continues.
The problem, however, goes deeper. It appears that the way the incomplete maternal mortality data that serves as a basis for the estimations is produced receives little to no scrutiny. It seems that such data, which countries report to international institutions and monitoring bodies, is accepted as it is. This is obviously problematic.
Research indicates that the production of MMR figures is highly political and that this is affecting the integrity of nascent systems that produce partial data in some countries. This calls for attention.
To demonstrate, studies in Ethiopia show how the state’s political ambition to project itself as an example of a raising, developmental economy results in the production of health data, particularly maternal death data, which is tailored more to mirror the desired image rather than the reality. This comes in different forms, including intentional underreporting of maternal deaths. In this regard, Andrea and colleagues (2019) found that health managers pressure health workers to report fewer maternal death numbers than actually identified or simply chose not to report maternal deaths further. This is informed by the fact that evaluation of their performance, which is essential for their further career development and other benefits, takes maternal mortality as a key factor.
In Malawi, a strong association between reported MMR and the political legitimacy of successive governments drives distortions in the integrity of the data production process (Wendland, 2016). Adrienne Strong (2020) has also documented how health workers in Tanzanian health facilities manipulate health data documentation as a way of defending themselves against personal accountability scares.
Health data is political, not only because it can be used for various political ends, but also because, informed by this knowledge as shown above, its very production can be compromised. It appears that the latter aspect has not received the degree of attention it deserves.
Like other health data, the MMR for many countries is an interpretative construct, resulting from continuous negotiations on what to include and what not to. It is thus necessary to pay attention to the environment within which reported maternal health data is produced. Efforts that aim to support countries in developing workable routine health information systems should duly consider the need to maintain the integrity of systems against extraneous interests.
In this regard, inbuilt mechanisms in the human rights systems, which focus on the transparency of data production processes, can be useful. Directing and supporting civil societies and the media to push governments to account for such critical numbers, rather than taking reported numbers for granted, may help. Empowering health workers to claim their rights also has the potential to minimize excessive political interference. Such endeavors would, moreover, reinforce a much-needed move to strengthen the downward accountability of countries to their citizens.
References
Clair L. Wendland, Estimating Death: A Close Reading of Maternal Mortality Metrics in Malawi IN Adams, Vincane (Ed.) Metrics: What Counts in Global Health (Duke University Press, 2016): 57–81.
Alicia Ely Yamin & Kathryn L. Falb, Counting What We Know; Knowing What to Count, 30 Nordic J. Hum. Rts. 350 (2012).
Katerini T. Storenga,d and Dominique P. Béhague, Guilty Until Proven Innocent”: The Contested Use of Maternal Mortality Indicators in Global Health, Critical Public Health, Vol. 27(2) (2017): 163–176.
Melberg, Andrea et al, Maternal Deaths Should Simply be 0’: Politicization of Maternal Death Reporting and Review Processes in Ethiopia, Health Policy and Planning, 34 (2019): 492–498.
Østebø, MT et al, The Silencing of Political Context in Health Research in Ethiopia: Why it Should be a Concern. Health Policy and Planning 33 (2018): 258–70.
Strong, Adrienne E., Documenting Death Maternal Mortality and the Ethics of Care in Tanzania (University of California Press, 2020).
UN Office of the High Commissioner for Human Rights, ‘Human Rights Indicators: A Guide to Measurement and Implementation’ (2012).
WHO et al, ‘Trends in maternal mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDP’ (2019).