Building the world’s first global map of podoconiosis
Dr Kebede Deribe, an epidemiologist at the Brighton and Sussex Medical School, has been leading efforts to create a global map of podoconiosis, a neglected tropical disease which was only formally identified less than thirty years ago. The Global Atlas will provide public health officials and policy makers with vital information needed to treat patients and to plan its elimination.
Dr Kebede Deribe’s first introduction to podoconiosis occurred in 2003 while managing an outpatient department in a rural health centre in southern Ethiopia. “A woman with leg swelling and a very sad face came to my department in the health centre. I was supposed to treat her”, said Deribe speaking on the phone from Addis Ababa. “The major cause of leg swelling that I knew about in tropical areas was lymphatic filariasis. I told her that I could treat her with a medication. In fact, it wasn’t correct advice.”
Luckily she couldn’t find the medication in the local pharmacies so Deribe sent her to a hospital in Addis Ababa where she was diagnosed with podoconiosis, a type of elephantiasis (leg swelling) found in subsistence farming communities in the tropics. When she returned, she visited the health centre and shared her case notes with Deribe.
It wasn’t Deribe’s fault that he couldn’t diagnose podo. During the four year health officer training that he and his fellow students received on both clinical care and public health training at that time, podo wasn’t mentioned once.
“I had never heard of podoconiosis before. Even in my undergraduate studies we were not taught about it. So I started to read about it and became interested in working on podo.”
 Foot hygiene is an important part of the treatment plan for the management of podo, as is wearing shoes, and bandaging and elevating the feet to reduce swelling. Credit: Kebede Deribe
Foot hygiene is an important part of the treatment plan for the management of podo, as is wearing shoes, and bandaging and elevating the feet to reduce swelling. Credit: Kebede Deribe
Even the World Health Organization only added podoconiosis to its list of neglected tropical diseases in 2011 due, partly, to the efforts of a research team led by Gail Davey, a Professor of Global Health Epidemiology at the Brighton and Sussex Medical School. It was while working at the School of Public Health in Addis Ababa for nine years that Davey heard about the disease and initiated a research programme into podo in 2005.
“I was first introduced to people affected by podoconiosis in 2002,” says Davey. “I was asked to review a small Ethiopian non- governmental organisation providing treatment and care for patients affected. I realised that there was nobody doing any research into this condition anywhere in the world.”
The disease generally occurs in areas with volcanic soils where subsistence farmers work in the fields barefoot. People with podoconiosis can have painful, swollen and deformed feet and legs and are often ostracised by their communities and excluded from school or social events because the causes of the disease are not widely understood.
Getting
podoconiosis
mapped

People living with
podoconiosis (podo) have
painful, swollen
and deformed
feet and legs¹
$208
million
per year
the estimated cost of
podo in Ethiopia
from lost productivity
and medical costs
based on a 2005
economic study²
Around
4 million
people
living in 32 countries
worldwide are living with podo³

2,357
the number of
locations where
data have already
been collected
29
the number of
countries that still
need to be
mapped³

The global
atlas of
podoconiosis
will end the guesswork
and form the basis for
treatment action plans⁴
- References
1. Davey G, GebreHanna E, Adeyemo A, Rotimi C, Newport M, Desta K: Podoconiosis: a tropical model for gene-environment interactions? Trans R Soc Trop Med Hyg 2007, 101(1):91-96.
2. Tekola F, HaileMariam D, Davey G: Economic costs of endemic non-filarial elephantiasis in Wolaita Zone, Ethiopia. Tropical Medicine & International Health 2006, 11(7):1136-1144.
3. Deribe K, Cano J, Trueba ML, Newport MJ, Davey G: Global epidemiology of podoconiosis: a systematic review. PLoS Negl Trop Dis 2018, 12:e0006324.
4. Deribe K, Cano J, Newport MJ, Pullan RL, Noor AM, Enquselassie F, Murray CJ, Hay SI, Brooker SJ, Davey G: The global atlas of podoconiosis. Lancet Glob Health 2017, 5(5):e477-e479.
I was first introduced to people affected by podoconiosis in 2002. I realised that there was nobody doing any research into this condition anywhere in the world.”Gail Davey
Professor of Global Health Epidemiology at Brighton and Sussex Medical School
With his interest sparked, Deribe decided to do a Master’s on podoconiosis and emailed Davey with some questions. This led to a PhD from The Brighton and Sussex Medical School (BSMS), which has become a global hub in podo research. Now a spatial epidemiologist with the Brighton and Sussex Medical School, Deribe is working on developing a Global Atlas of Podoconiosis through a five-year grant from the Wellcome Trust.
Mapping podoconiosis in Africa
Globally there are around 4 million people from over a possible 32 countries around the world living with podoconiosis, mainly in tropical countries of Africa, Central and South America, and Southeast Asia. But these are just estimates. The Global Atlas will help fill crucial gaps in knowledge.
So far, Deribe and his team have mapped three African countries – Ethiopia, Cameroon and Rwanda – and collected data from several others. Emerging evidence suggests that podo may no longer be endemic in certain countries in Africa, Asia and Latin America. By combining the data with the evidence, the number of countries which require mapping will be significantly reduced. In some of the countries the disease might already have been eliminated.
Deribe led the mapping process, developed the study design and sampling approach, conducted training on interview techniques, the mapping process and the use of smartphones to record and transmit data.
Over 141,238 individuals were tested in Ethiopia alone. The team surveyed more than 1,442 communities, screening 100 individuals within each community for leg swelling and for antigens. The testing is done to exclude lymphatic filariasis, which has similar symptoms to podo, such as swollen legs and feet, but is caused by parasitic worms, which are spread by the bite of infected mosquitoes. All of the surveys were conducted through Wellcome Trust funding using smart phones purchased through the grant.
 A health worker takes a blood sample as part of the podo screening programme. Credit: Kebede Deribe
A health worker takes a blood sample as part of the podo screening programme. Credit: Kebede Deribe
This survey data was combined with environmental data by Deribe and collaborators from the London School of Hygiene and Tropical Medicine and the University of Lancaster using a machine learning and geostatistical approach to develop estimates of the distribution of podoconiosis. The estimates take into account environmental and climatic factors responsible for the type of soil, such as altitude, rainfall and vegetation because podoconiosis is triggered, not by any bacterium, virus or parasite, but by an abnormal reaction to irritant mineral particles found in volcanic soils.
The mapping revealed marked differences between the three African countries. In certain areas of Ethiopia with volcanic soils prevalence can be as high as 4%, with around 1.5 million people living with podo out of an overall population of around 100 million. In Cameroon the prevalence is lower (around 0.5%), but it’s widespread, with around 42,000 people living with podo. It is also endemic in all 30 districts of Rwanda, with an estimated 6,429 living with the painful disease.
“Mapping is the first step”
Currently only 3% of those people living with podo are accessing the treatment they need and deserve. Mapping could help identify other regions and groups of people at risk of living with the disease.
“Mapping is the first step for delivering an intervention,” said Deribe. “It’s a decision tool. In Ethiopia our advocacy efforts were fruitful because we know which districts are affected and we can tell
partners, implementers and donors where to invest their resources to tackle podo.”
The map of podo in Ethiopia was used by the Ethiopian Ministry of Health to develop a national master plan for neglected tropical diseases for 2016 – 2020 and used in long-term health plans, such as their health sector transformation plan.
Mapping
podoconiosis
in Africa
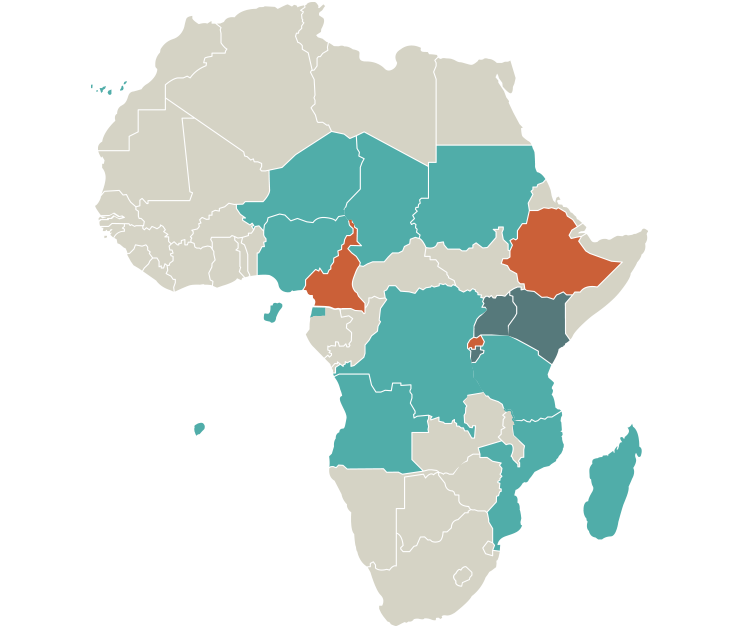
Ethiopia
1,537,963
affected people¹
Cameroon
41,556
affected people²
Rwanda
6,429
affected people³
Uganda
Kenya
Burundi
Mapped
To be mapped
Suspected endemic: Angola, Cape Verde, Chad, Democratic Republic of Congo, Equatorial Guinea, Madagascar, Mozambique, Niger, Nigeria, Sao Tome and Principe, Sudan, Tanzania
Most affected
countries

Ethiopia
1,537,963
affected people¹

Cameroon
41,556
affected people²

Rwanda
6,429
affected people
- References
1. Deribe K, Cano J, Giorgi E, Pigott DM, Golding N, Pullan RL, Noor AM, Cromwell EA, Osgood‐Zimmerman A, Enquselassie F et al: Estimating the number of cases of podoconiosis in Ethiopia using geostatistical methods. Wellcome Open Res 2017, 2(78).
2. Deribe K, Cano J, Njouendou AJ, Eyong ME, Beng AA, Giorgi E, Pigott DM, Pullan RL, Noor AM, Enquselassie F et al: Predicted distribution and burden of podoconiosis in Cameroon. BMJ Glob Health 2018, 3(3):e000730.
3. Deribe K, Mbituyumuremyi A, Cano J, Mbonigaba et al: Geographical distribution and prevalence of podoconiosis in Rwanda: a cross-sectional country-wide survey. The Lancet 2019.
Mapping is the first step for delivering an intervention. It’s a decision tool.”Dr Kebede Deribe
Epidemiologist at the Brighton and Sussex Medical School
The maps help public health managers and policy makers understand the way the disease is linked to a country’s geography. “Maps are quite attractive and intuitive,” said Davey. “When we can show governments clear figures and distribution patterns, they have the information on which to base policy.”
They also help galvanise much-needed resources and expertise. “Mapping is used as an important advocacy tool to mobilise resources once the extent of the problem and distribution of the disease is known,” said Deribe. “Donors want to invest in diseases that are clearly understood – both in terms of the geographical distribution and the burden estimates.” Maps also provide important benchmarks for evaluating efforts to eliminate the disease.
Pan-African collaboration
The Global Atlas project is also building skills, long term partnerships and Pan-African collaboration needed for podo’s elimination. “Our partners have the understanding of the local context and presence on the ground and we have technical expertise on podoconiosis and on mapping,” Deribe said. “When we map podo, we bring these two things together.”
 A man with podo being interviewed by a health worker during a survey of a community in Musanze, a mountainous district in northern Rwanda. Credit: Kebede Deribe
A man with podo being interviewed by a health worker during a survey of a community in Musanze, a mountainous district in northern Rwanda. Credit: Kebede Deribe
This collaboration extends beyond the mapping. Deribe recently went with a team of podoconiosis experts from Ethiopia to train health workers in Cameroon and Uganda on the management and treatment of patients with podo, known in medical parlance as ‘morbidity management’. They soon plan to carry out a similar training in Rwanda with health professionals there.
“When Dr Kebede goes into a country, he’s there not just to do the technical side of mapping but to start building the partnerships that will help deliver the programmes to help patients,” says Davey. “The Global Atlas is really important for building those partnerships – the two things go hand in hand.”
Global Atlas: what gaps remain?
The sheer ambition of the Global Atlas is formidable. Whole continents, including Latin America and India, are currently blank on the Global Atlas, but progress is being made. In 2019 alone, Deribe is planning to conduct nationwide mapping in Burundi, Uganda and Kenya. His team have also begun collaborating with Indian institutions to begin developing a plan for mapping podo in India.
He has also set his sights on Latin America. “Looking forward we would like to confirm whether podo exists or has been eliminated from Latin America,” says Deribe. “Initial assessment in Guatemala suggest the absences of podoconiosis. If it exists we have to go and map it. If it doesn’t exist that would be another important story to document: how it was eliminated without any outside intervention.”
Author: Suzanne Fisher-Murray, University of Sussex
Date published: 7 May 2019
Infographic development was funded by the ESRC Impact Acceleration Account.
Contact us
Research development enquiries:
researchexternal@sussex.ac.uk
Research impact enquiries:
rqi@sussex.ac.uk
Research governance enquiries:
rgoffice@sussex.ac.uk
Doctoral study enquiries:
doctoralschool@sussex.ac.uk
Undergraduate research enquiries:
undergraduate-research@sussex.ac.uk
General press enquiries:
press@sussex.ac.uk